Basic HTML Version


Chapter 11
8
!
Treatment.
A pneumothorax requires
urgent medical attention
. The extent of lung collapse is assessed
clinically and confirmed by a chest x-ray. A large pneumothorax is treated by placing a
tube
into the pleural air space
and connecting it to a one-way valve such as a Heimlich valve or
an underwater drain. This allows air out of the pneumothorax but prevents its return. The
placement of tubes in the chest is usually beyond the capability of untrained personnel as
there are important structures, like the heart, which can be injured in the process. After a
period of hours or days the tear in the lung usually heals and the lung slowly re-inflates.
A minor pneumothorax (less than 25% lung collapse) may be treated by the diver
breathing
100% oxygen
(see Chapter 40).
A
tension pneumothorax
is a medical
emergency
. The pressure in the pneumothorax must
be relieved by the insertion of a needle or tube through the chest wall, into the
pneumothorax.
If the diver is aware of the possibility of a pneumothorax, he may be able to alert a physician
to the possible diagnosis if any of these clinical features are present. The physician may
release the air by inserting a needle into the second intercostal space in the mid-clavicular
line, or through the 5–6 intercostal space in the mid-axillary line. Both have potential
complications.
Air Embolism
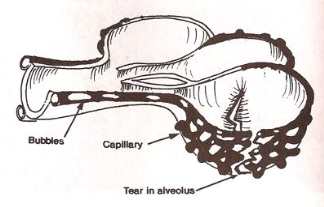
When the lungs rupture, tears in the alveoli walls (and contained blood capillaries) can allow
air to enter the blood circulation. This air is conducted to the left side of the heart, from
whence it is pumped through the arterial circulation.
Fig. 11.6
Diagram of a ruptured alveolus and capillary vessel from pulmonary
barotrauma of ascent. Air bubbles (emboli) are entering the veins carrying
blood back to the left atrium of the heart.